Combined Oral Contraceptives (COC) and Progestin-Only Pills (POP)
Combined oral contraceptives (COCs), which were approved in June 1999 and launched the same year in September, contain estrogen and progestin as their main components and have been used in Japan for 26 years. In order to maintain contraceptive effectiveness while reducing side effects, research has focused on minimizing hormone doses as much as possible to reduce the burden on the body. This has resulted in the low-dose pills we know today. They are referred to as "combined" oral contraceptives because they are made from two hormonal agents. Because combined oral contraceptives contain estrogen, however, there were concerns about risks such as thrombosis. As such, in 2025, a progestin-only oral contraceptive (POP) was approved and launched in Japan as well.
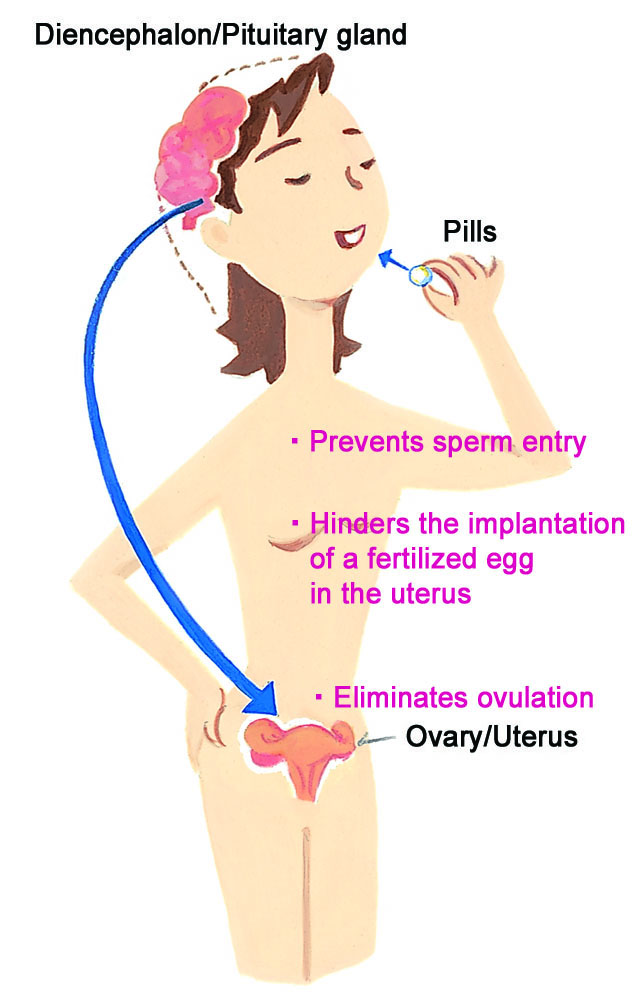
●How the Pill Prevents Pregnancy
Both COCs and POPs exert their contraceptive effects through multiple mechanisms of action mediated by the female hormones contained in the tablets, including: (1) suppression of ovulation, (2) thinning of the endometrium, and (3) inhibition of sperm penetration due to increased viscosity of cervical mucus. The contraceptive effectiveness of COCs and POPs is considered to be roughly equivalent (see page 12).
●Usage Guideline for Low-Dose Pills
Oral contraceptives, being hormone-based medications, require a doctor’s prescription and will be provided only if deemed suitable by your healthcare provider.
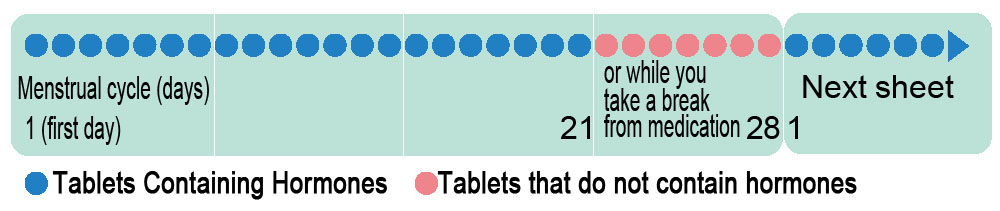
●How to take the pills
When starting either COCs or POPs for the first time, take the first pill on the first day of menstruation. There is a risk of pregnancy if you start later than the first day of menstruation. As such, be sure to use another contraceptive method during the first week after starting the pill.
COC pills are available in 21-tablet or 28-tablet packs. With the 21-tablet pack, you take one pill daily for 21 days, followed by a 7-day break. You then start a new pack on the 8th day. For the 28-tablet pack, the final 7 pills are placebo tablets, so you will directly commence a new pack the day after the last (28th) tablet. Expect menstrual-like bleeding during the 7-day break for the 21-tablet pack or while taking the placebo pills during the final 7-days for the 28-tablet pack.
The POP currently available in Japan is a 28-tablet pack, consisting of 24 active tablets and 4 placebo tablets, which are taken in a repeating cycle. In many cases, menstruation-like bleeding occurs during the placebo phase; however, withdrawal bleeding may sometimes be absent. If bleeding does not occur for two consecutive cycles, a pregnancy test may be recommended.
Additionally, there are hormonal medications available that alleviate pain associated with endometriosis and treat painful menstruation (dysmenorrhea). Although they are not used strictly as contraceptives, they still offer contraceptive benefits.
●When you forget to take the pill
If you miss a COC dose (other than a placebo) and you only notice the next day, take it as soon as you remember, then take that day's tablet as usual as well. If you forget to take the pill for two or more consecutive days, stop taking it, and wait for your next menstruation to begin a new pack.
If you miss a POP dose (other than a light yellow tablet), and you only notice the next day, take it as soon as you remember, then take that day's tablet as usual as well. If you forget to take the pill for two or more consecutive days, stop taking it, and wait for your next menstruation to begin a new pack.
●Characteristics of progestin-only oral contraceptives (POPs)
Because COCs contain estrogen, their use has often been subject to restrictions. The POP launched in June 2025 is a type of progestin formulation in which 4 mg of drospirenone is taken for 24 days, followed by 4 days of placebo tablets, in a repeating cycle. Menstruation-like bleeding typically occurs during the placebo phase (though it may not occur in some cases).
Drospirenone is thought to enhance contraceptive effectiveness through multiple mechanisms of action, including suppressing ovulation through its progestogenic activity, inhibiting sperm penetration through increased viscosity of cervical mucus, and inhibiting egg implantation through thinning of the endometrium. The pregnancy rate was reported to be 0.36%. This is comparable to the annual pregnancy rate of 0.29% observed with pills developed in Japan.
According to the WHO publication, "Medical eligibility criteria for contraceptive use," POPs are recommended not only for women at risk of thrombosis, but are also listed as having "no restriction for use" in relation to age, smoking, breastfeeding, or high blood pressure (provided it is well-controlled). It is poised to gain increasing attention as a safe and reliable contraceptive option for Japanese women seeking dependable protection.
Hormonal Content in Low-Dose Pills Compared
Low-dose contraceptive pills are designed with a reduced concentration of estrogen (follicle hormone), typically containing between half to three-quarters of the estrogen found in medium and high-dose options. Simultaneously, the formulation enhances the effectiveness of progesterone while also lowering its quantity.
Hormonal Levels in low-dose pills (for contraceptive purposes) and medium- and high-dose pills
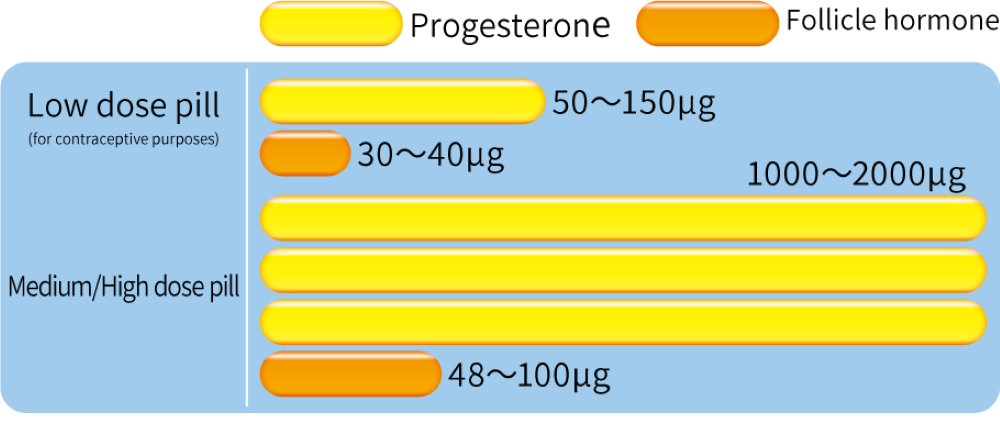
*Low-dose pills are generally characterized by having less than 50μg of follicular hormone.
Hormonal Content in Low-Dose Pills Compared
Non-contraceptive benefits of COC pills
■Regulation of menstrual cycles for those with irregular periods, promoting consistency.
■Reduction in menstrual flow, which can help prevent and alleviate iron deficiency anemia.
■Alleviation of menstrual cramps.
■Improvement in acne conditions.
■Decrease in the risk of ectopic pregnancies.
■Lowered incidence of endometrial and ovarian cancers.
The cancer risk reduction benefit persisting even after stopping the pill.
■Reduction in the risk of colorectal cancer, a leading cause of cancer death among women.
Who should avoid COC pills
■Individuals with high blood pressure, or those with heart, liver, or kidney disease.
■Those who have experienced thrombosis or are at high risk for it.
■Individuals around the time of elective surgery (such as abdominal or orthopedic surgery).
■Those with unexplained genital bleeding.
■Individuals suspected of having malignant tumors in their genitals or breasts.
■Heavy smokers over the age of 35 (consuming 15 or more cigarettes daily).
■Pregnant individuals or those who may be pregnant.
■People within 3 weeks postpartum.
■Those within 6 months postpartum who are breastfeeding and wish to continue.
Varieties of Low-Dose Pills
Low-dose contraceptive pills are categorized into two types: one with a pack of 21 tablets and another with 28 tablets. The pack of 21 consists entirely of hormonal pills, whereas the 28-tablet pack includes 7 placebo tablets, which are hormone-free, to aid in maintaining the habit of daily intake.
●Guidance on Using the 21 or 28 Tablet Packs:
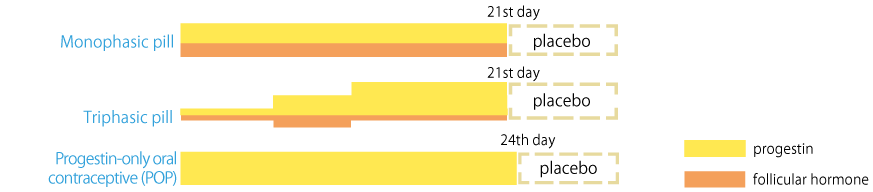
Besides varying pill counts and types, there are three-stage pills that gradually adjust hormone levels and others that offer enhanced progesterone effects.
●Monophasic pill (COC) Every tablet within a single pack has an identical hormone dosage.
●Triphasic pill(COC) This version modifies the hormone dosage in three stages throughout one pack. Some increase hormone levels mid-pack, while others elevate progressively at each stage.
●Progestin-only oral contraceptive (POP) In 2025, an oral contraceptive containing only progestin was approved and made available in Japan. It may be used without restrictions related to age, smoking, or obesity, or high blood pressure (provided it is well-controlled). Please consult your doctor for more information.
(example)
FAQ
QCan I Use the Pill If I Smoke?
AResearch from various countries indicates that smokers over the age of 35 who use the pill face a higher risk of myocardial infarction compared to non-smokers. Therefore, it's advisable to quit smoking if you plan to start the pill.
To begin with, smoking has a negative effect on the body.
QIs It Safe to Take the Pill While Breastfeeding?
ASince traditional birth control pills can reduce breast milk production, they might make breastfeeding challenging. If you're keen on continuing to breastfeed, it's recommended to avoid the pill for the first 6 months postpartum. However, progestin-only pills (POP) can be taken immediately after giving birth. Please consult with your health care provider to go over your options.
QCan the Pill Address Menstrual Issues?
AThe pill's active components, progesterone and estrogen, can alleviate conditions like painful menstruation, heavy menstrual flow, and irregular cycles. This improvement is attributed to the pill's ability to suppress ovulation, leading to a thinner uterine lining and consequently less bleeding and fewer uterine contractions during menstruation.
Additionally, the pill helps regulate menstrual cycles, offering stability for those with irregular periods.
QHow should I handle leftover pills I forgot to take?
AIf you've missed some doses and have leftover pills, those with a consistent hormone level can be utilized if you aim to slightly delay the start of your menstrual period by 2 to 3 days. For pills with varying hormone levels or if you're left with placebos, it's advisable to dispose of them, as their contraceptive efficacy may be compromised.
Remember, the pill's effectiveness hinges on correct and consistent use.
QCan the pill prevent diseases such as AIDS?
AThe pill does not offer protection against sexually transmitted diseases (STDs), including AIDS. To prevent infection, especially if there's any risk, combining the use of condoms with the pill is recommended for comprehensive protection.
QHow long should I stop taking the pill if I want to have another child?
AThere's no mandatory waiting period before trying to conceive. Ovulation typically resumes normal patterns for 90% of individuals within three months after stopping the pill.
IUD・IUS
An IUD (intrauterine device) is a small device inserted into the uterus for birth control. There are plastic IUDs as well as IUSs (progestin-releasing systems) with added progestin.
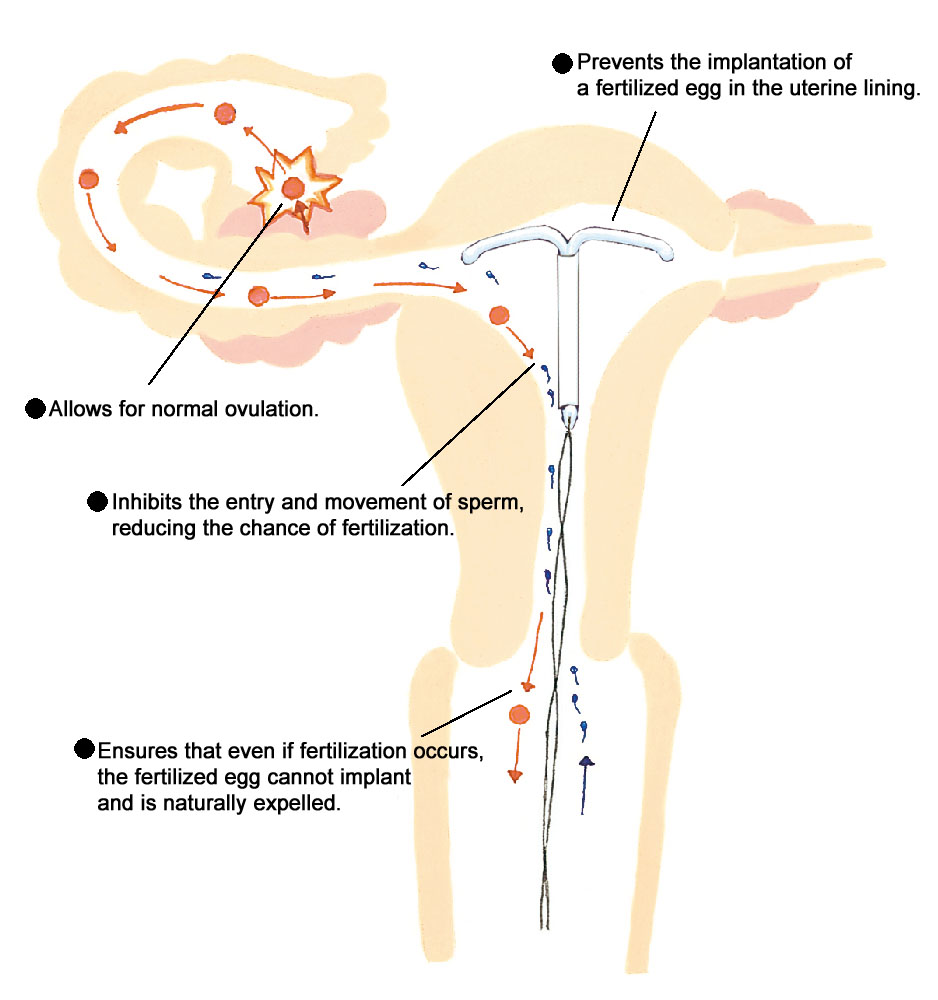
IUDs hinder sperm mobility and block them from reaching the fallopian tubes, altering the uterine environment to prevent egg implantation, with copper IUDs believed to be particularly potent. Nonetheless, Japan will cease production of copper IUDs in 2023, removing them from the market by 2024.
On the other hand, the IUS releases a modest amount of progesterone daily, which directly influences the endometrium by inhibiting its growth, obstructing the implantation of fertilized eggs, and also thwarting the entry of sperm into the uterus. The progesterone from the IUS minimally enters the bloodstream, thus barely affecting ovulation and having negligible systemic impacts.
Types of IUD/IUS
Open type
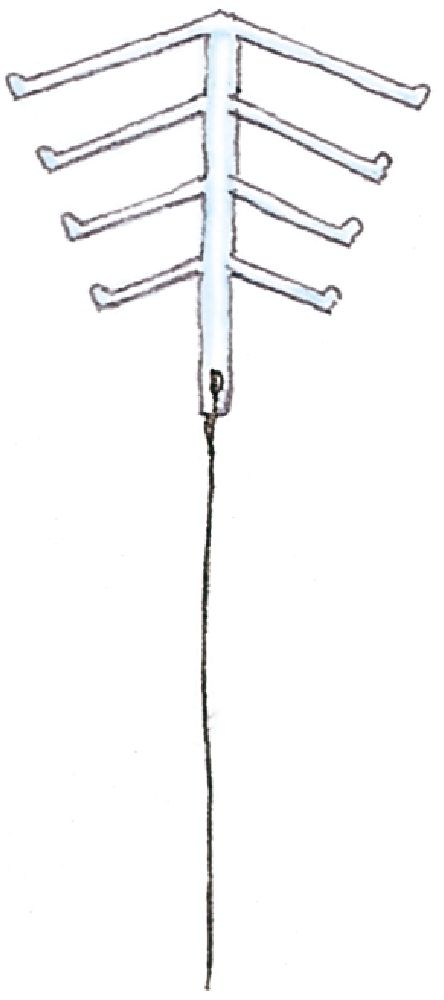
Open type
(IUS)

A thread is attached to the contraceptive device to allow for easy removal.
●Features
The IUD/IUS is designed as a slim, long plastic tube, allowing for insertion without the need for anesthesia, making the process more straightforward for both the patient and the healthcare provider. This design facilitates easy verification of proper placement and removal by physicians.
Open-type plastic IUDs have slightly weaker contraceptive effects, whereas the IUS is extremely effective. A notable benefit of the IUS is its ability to decrease menstrual flow.
Once placed, the device is intended to remain effective for about 5 years. Follow-up examinations typically occur one month, six months, and one year post-insertion. Assuming no complications arise, subsequent check-ups are advised every six months to a year.
●Installation:
An obstetrician-gynecologist will install the device following a thorough medical evaluation. Optimal timing for insertion is generally 3 to 7 days from menstrual onset or 6 weeks postpartum, once the uterus has reverted to its pre-pregnancy size. The device is also compatible with breastfeeding.
Insertion is performed on an outpatient basis without the need for anesthesia. For contraceptive use, health insurance coverage is not available, necessitating out-of-pocket payment.
However, since 2015, insurance coverage has been extended to include IUS for individuals experiencing heavy menstrual bleeding or severe dysmenorrhea.
Who is Suited/Not Suited for IUD/IUS
| Suitable for: |
■Individuals who have previously given birth. ■Those wishing to postpone their next pregnancy. ■People seeking long-term contraceptive solutions. ■Those who prefer not to use contraceptives on a per-occasion basis. ■Middle-aged and older individuals. ■Individuals experiencing heavy menstrual flow. (in the case of IUS) |
|---|---|
| Not Suitable for: |
■Individuals who have never given birth. ■Those with heavy menstrual bleeding (in the case of IUD) ■People at a higher risk of acquiring sexually transmitted diseases from multiple partners. ■People with deformities in the uterine cavity ■Those currently experiencing genital inflammation. ■Individuals with suspected cervical or ovarian cancer. |
IUD/IUS contraceptive mechanism
FAQ
QIs it painful to insert an IUD?
AInsertion may cause a brief moment of discomfort, but the devices are designed for smooth placement to minimize this. Both copper IUDs and IUS devices are small and typically cause no discomfort once in place.
QWill having an IUD or IUS affect my menstruation?
AMenstrual cycles continue as normal. Post-IUD insertion, you might notice slight spotting between periods or a minor extension in menstrual length. An IUS may significantly reduce menstrual flow and alleviate cramps, although light, irregular bleeding could occur for 1 to 3 months following insertion. These changes are generally not a cause for concern.

Emergency Contraception
As of March 2026
Emergency contraception serves as a crucial option in the event of unprotected sex, condom failure, withdrawal failures, or assault. Emergency oral contraceptives need to be taken within 72 hours, and a copper IUD or IUS (intrauterine system) can be inserted up to 120 hours after the incident. You can receive these contraceptives by visiting a healthcare provider; starting from February 2, 2026, you can also receive emergency contraceptives over the counter from pharmacies, as long as you meet certain requirements.
Remember, emergency contraception is not meant for regular use but as a measure for unexpected situations. Domestic clinical trials have indicated that the efficacy of emergency contraceptive oral pills is only 81%, highlighting that it is not entirely foolproof. For regular contraception, consider low-dose pills.
●How to take them
In Japan, the available emergency contraceptives are "Norlevo Tablets 1.5mg" and "Levonorgestrel Tablets 1.5mg 'F'." Over-the-counter options are "Norlevo" and "Lesoel 72." Take one tablet at a time.
●Note
• Engaging in intercourse post-medication without contraception could result in pregnancy.
• Post-consumption, side effects such as unusual uterine bleeding, headaches, nausea, fatigue, and drowsiness may occur.
• If vomiting occurs within 2 hours of ingestion, an additional dose should be taken immediately.
• The absence of pregnancy is suggested by menstruation-like bleeding after taking the medication. However, a doctor's visit is advised regardless of bleeding to confirm non-pregnancy.
• Emergency contraceptives do not offer protection against sexually transmitted infections, including AIDS.